The Evidence Is In: Covid Deaths Were Faked in order to Panic People into Accepting Injection with an Unknown Substance called a “vaccine”

He wrote the following on this webpage:
We are all used to the Government lying but in my view this has to be one of the biggest lies of all.
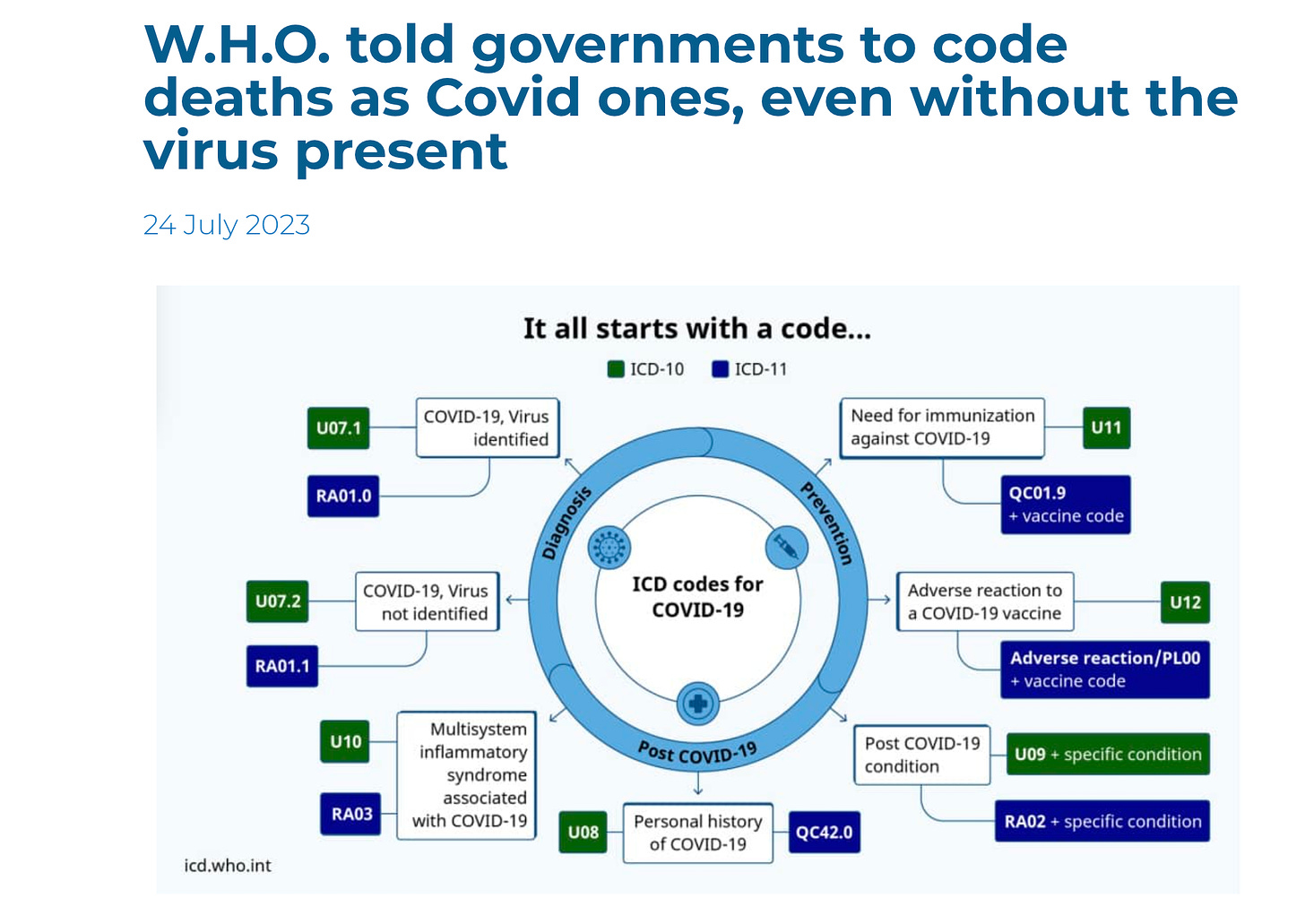
The World Health Organisation has told governments to code deaths to Covid even if the virus was not identified in an autopsy and even if it was not medically correct.
And I quote page 8 of the attached link below:
“Although both categories, U07.1 (COVID-19, virus identified) and U07.2 (COVID-19, virus not identified) are suitable for cause of death coding, it is recognized that in many countries detail as to the laboratory confirmation of COVID-19 will NOT be reported on the death certificate. In the absence of this detail, it is recommended, for mortality purposes only, to code COVID-19 provisionally to U07.1 unless it is stated as “probable” or “suspected”.
The international rules and guideline for selecting the underlying cause of death for statistical tabulation apply when COVID-19 is reported on a death certificate but, given the intense public health requirements for data, COVID-19 is not considered as due to, or as an obvious consequence of, anything else in analogy to the coding rules applied for INFLUENZA. Further to this, there is no provision in the classification to link COVID-19 to other causes or modify its coding in any way.
With reference to section 4.2.3 of volume 2 of ICD-10, the purpose of mortality classification (coding) is to produce the most useful cause of death statistics possible. Thus, whether a sequence is listed as ‘rejected’ or ‘accepted’ may reflect interests of importance for public health rather than what is acceptable from a purely medical point of view. Therefore, always apply these instructions, whether they can be considered medically correct or not. Individual countries should not correct what is assumed to be an error, since changes at the national level will lead to data that are less comparable to data from other countries, and thus less useful for analysis.”
Let’s not forget authorities in Australia wouldn’t recognise someone as being vaccinated until 21 days after the jab, meaning that many of the vaccine injured or deaths had their injury correlated to Covid not the jab.
This World Health Organization document quoted above proves that the world public health leadership at the WHO faked death reports during the pandemic. This was designed to overestimate the death rate worldwide.
This document, titled: “INTERNATIONAL GUIDELINES FOR CERTIFICATION AND CLASSIFICATION (CODING) OF COVID-19 AS CAUSE OF DEATH Based on ICD International Statistical Classification of Diseases” clearly demonstrates, with images no less, that the WHO was and IS requiring countries to jigger death certificates to code for more COVID-19 deaths than there actually were.
The document also “teaches” physicians and hospitals to code for COVID-19, even when the cause of death may have been something else. Note that in the WHO examples below, a positive COVID-19 test is not necessary for listing COVID-19 as the cause of death.
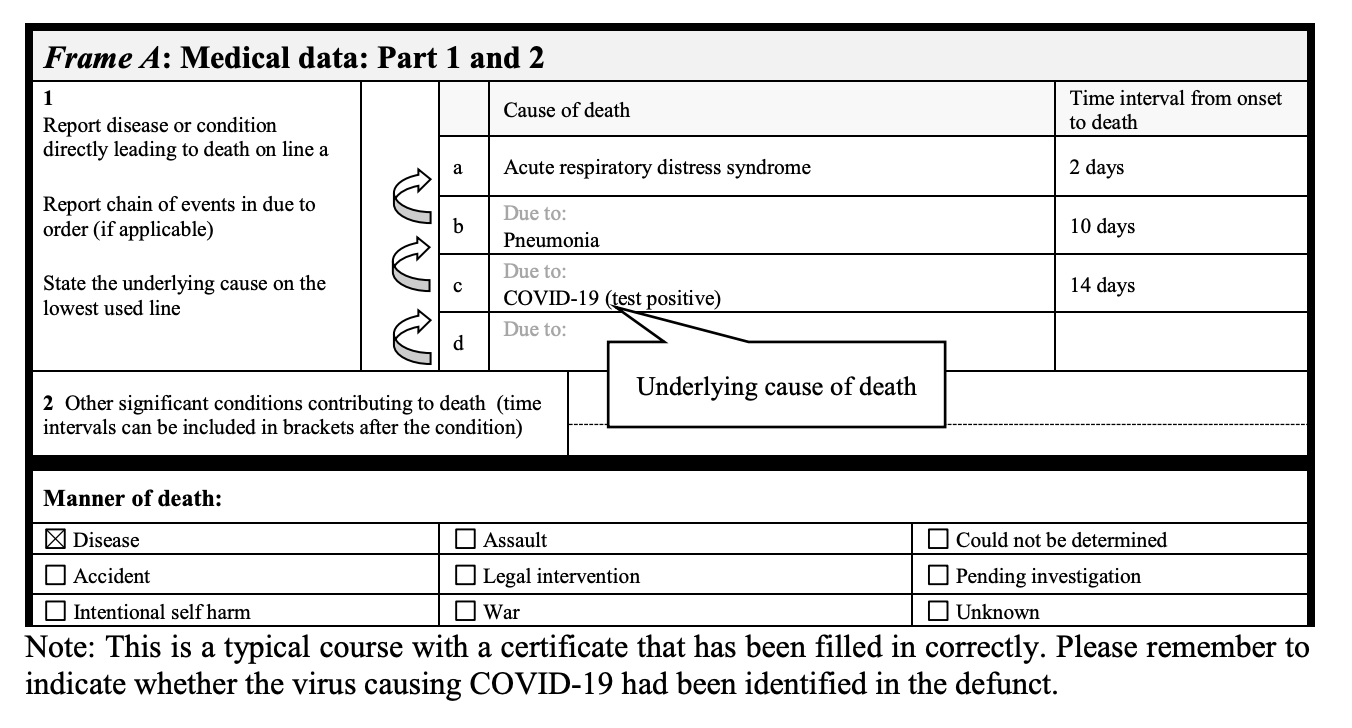
The first example from the document shows that if there is a positive test, the death certificate should be labelled as such. Without such labelling, there would not have been a positive test. This is what a positive COVID-19 test would look like on a death certificate.
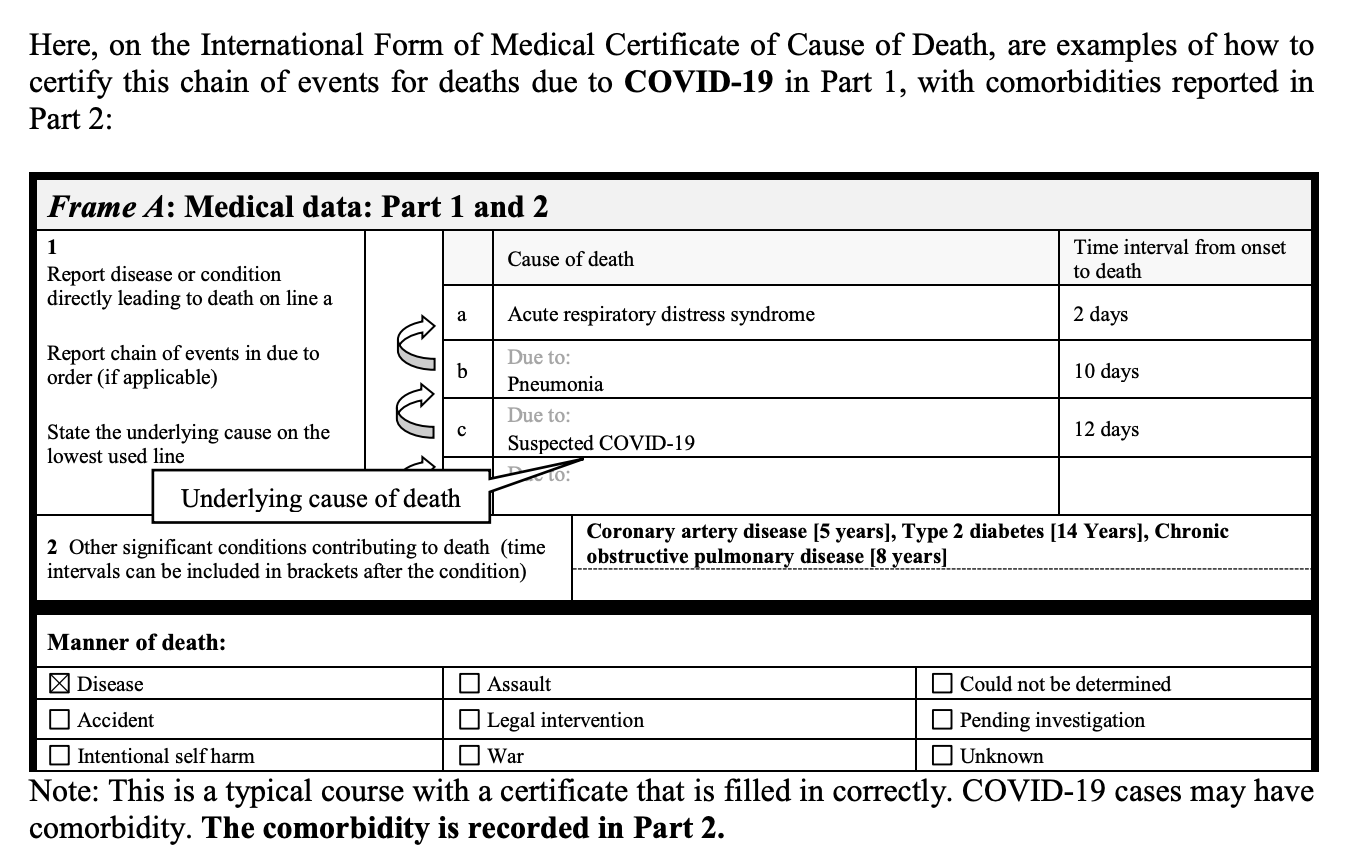
The example above documents that despite the fact that this patient had Coronary artery disease, type 2 diabetes, and COP – WHO advises that on the death certificate, COVID-19 be listed as the primary cause of death. Even without a positive test.
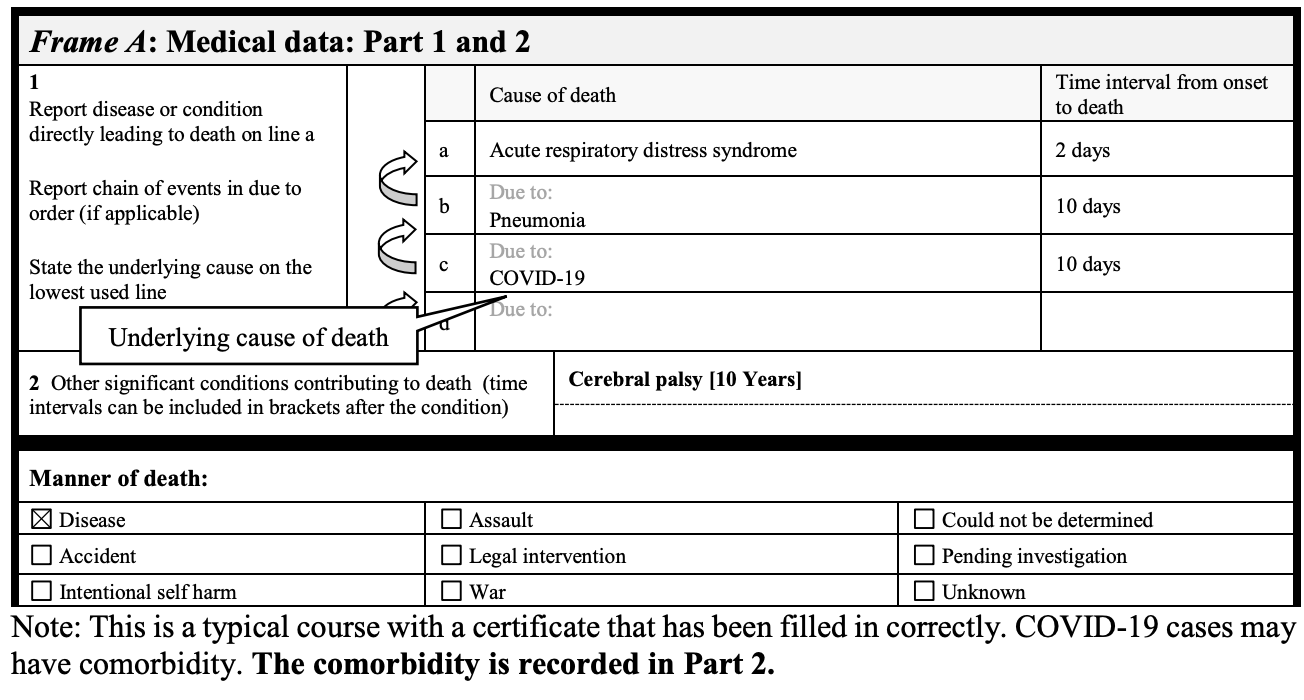
In another example, the patient had cerebral palsy – a disease that is associated with extremely high childhood death rates, yet without a positive test – that child was listed as a COVID-19 death.
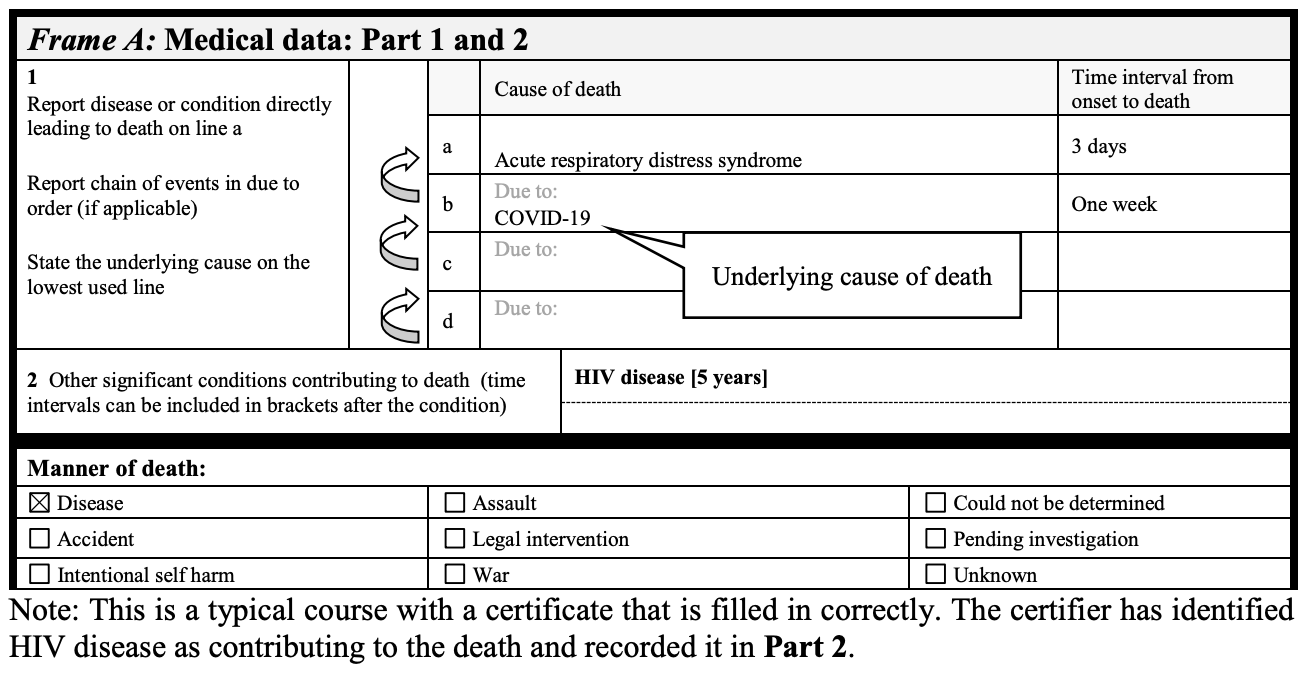
Likewise, this last example shows that a patient with HIV- and no positive test would be listed a COVID-19 death.
In the USA, this appears to get even more nefarious.
Due to the CARES act, medicare paid hospitals a 20% “add-on” to the regular payment for COVID-19 patients. Remember that the people who became sick from COVID were generally the elderly and on medicare. Ergo: the incentive to put people on ventilators. There was a financial incentive to put people on ventilators and yet ventilators contributed to many of the COVID-19 deaths.
It is less clear if hospitals actually received a payment from a government agency for a positive COVID-19 cause of death on the certificate (if anyone can find an actual government document stating that, I would love to see it).
Here is the NIH protocol for treating COVID-19 which hospitals were encouraged not to deviate from:
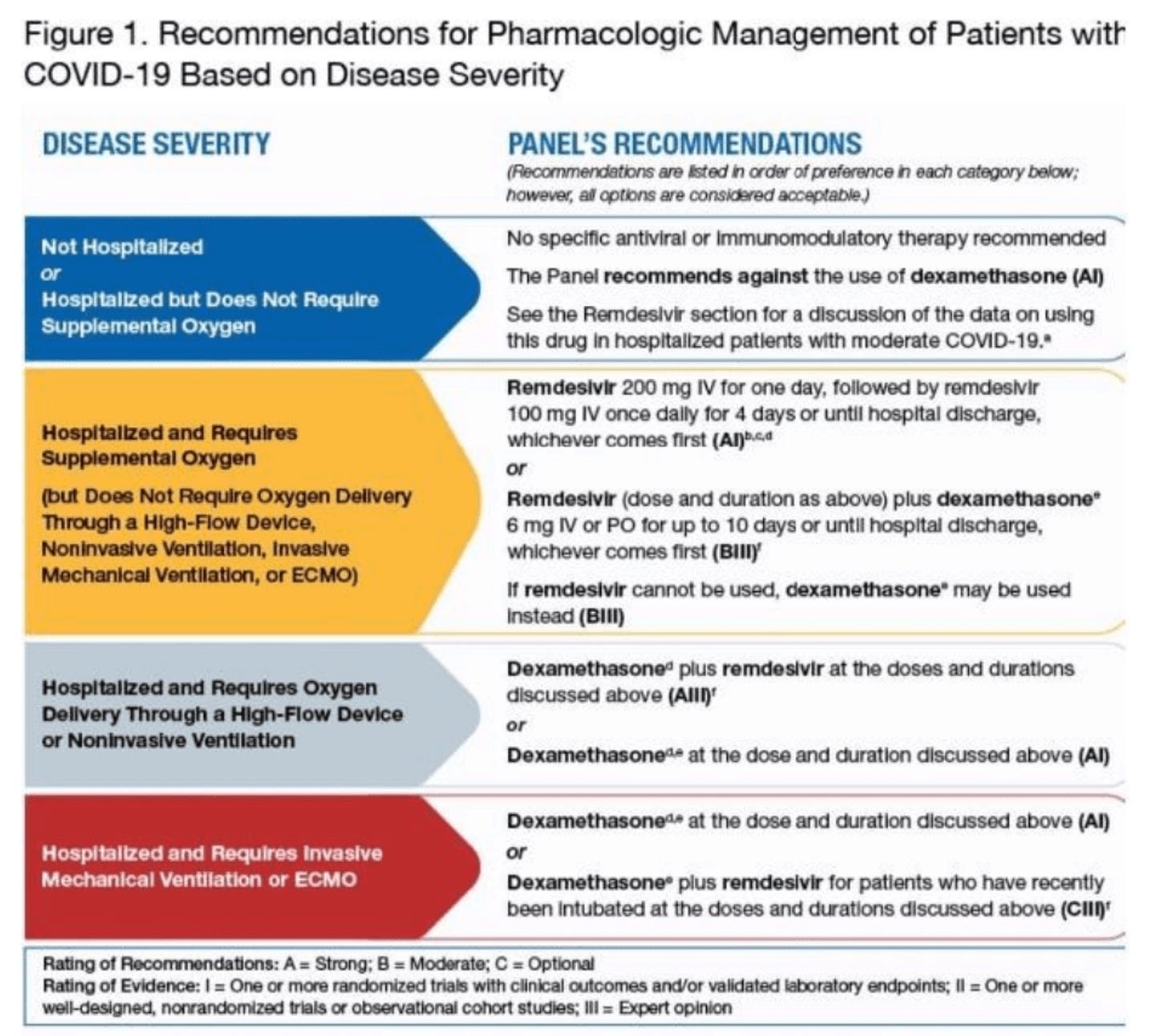
Note that remdesivir is still considered the main drug of choice for treating COVID-19 by the NIH, even in many patients with mild to moderate disease. Yet this drug is known for causing renal failure and significantly higher rates of death in various patient populations, such as those receiving high flow oxygen. Yet, the NIH guidelines above STILL recommend remdesivir for patients on high flow oxygen.
Do they want to kill people? It sure seems that way.
Revisiting this information is important, given that the WHO was and is encouraging countries throughout the world to code for COVID-19 deaths, even when some of those deaths most likely weren’t caused by COVID.
So, not only was the death rate over estimated worldwide, in the USA at least, ventilation and remdesivir were strongly “encouraged” by the government. The NIH was using treatment protocols that were intentionally or not, designed to kill people. These are strong words. Physicians were not allowed to deviate from these government protocols. Protocols that killed people.
This has led to a general mistrust of public health and rightly so.
It is evil to fake deaths to cause the mortality rates of COVID-19 to spike.
It is evil to force physicians to use protocols that were not clinically tested or proven to be effective.
Our public health system is broken worldwide and it is only getting worse.
No comments:
Post a Comment